Pediatric GI Clinical Toolkit
Recognizing and diagnosing EoE in children
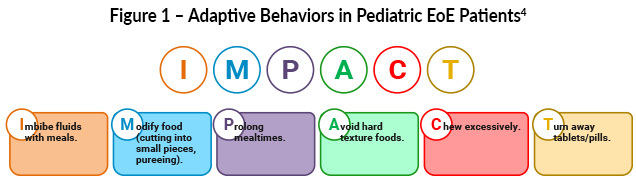
Identifying pediatric patients who should be further evaluated for EoE can be challenging, as symptoms are often non-specific, overlap with other common gastrointestinal conditions, especially gastroesophageal reflux disease (GERD), and vary by age. Younger children commonly present with nausea, vomiting, abdominal pain, feeding difficulties, or poor growth, whereas adolescents are more likely to experience dysphagia, heartburn, regurgitation, or food impaction. 1- 3 Patients with EoE develop adaptive behaviors that mask their dysphagia symptoms. The acronym IMPACT can help identify these adaptive behaviors (Figure 1).4
While interpreting endoscopic findings using the EoE reference score, EREFS (Edema, Rings, Exudate, Furrows, and Stricture), it is important to remember that esophageal strictures have been observed at much lower rates in pediatric EoE patients than in adults.5
Treatment of Pediatric EoE
Dietary therapy is a cornerstone of pediatric EoE treatment and targets food antigens driving eosinophilic inflammation.6 An elemental diet, although effective in achieving remission, presents challenges, such as poor adherence due to palatability, feeding skill regression, and significant burden on caregivers.7 In contrast, an empiric elimination diet is easier to implement, either using a step-up or top-down approach.7 When dietary changes are made, follow-up endoscopy with biopsy is important to confirm treatment effectiveness. Dietary therapies are effective first-line options in pediatric patients, and empiric elimination diets are advantageous because allergy testing is not pathognomonic for identifying food triggers. Pediatric patients managed with elimination diets should be referred to a registered dietitian if they experience excessive weight changes, poor adherence, compromised nutritional quality, or negative effects on quality of life.3
Pharmacologic therapy: In a randomized study of 64 pediatric patients, proton pump inhibitor (PPI) therapy alone has demonstrated histologic improvement, with no added benefit when combined with dietary elimination.8 PPIs are widely used due to favorable safety and tolerability.9 In a retrospective comparison of pediatric patients with a mean age of 10 years, the swallowed topical corticosteroid, viscous budesonide, was more effective than fluticasone propionate, with lower post-treatment eosinophil counts after eight weeks.10 Long-term data from a four-year phase 3 open-label study of budesonide oral suspension demonstrated sustained histologic response in approximately half of patients aged 11 years and older, with maintained endoscopic improvement and similar outcomes in children and adults.11 Growth impairment is uncommon with topical steroid therapy, and adrenal insufficiency is not considered a frequent adverse effect.4
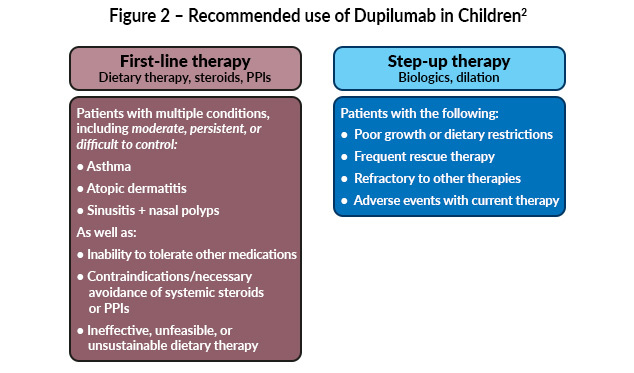
Targeted biologic therapy, dupilumab, was approved for adolescents aged ≥12 years in 2022 and expanded in 2024 to include children aged ≥1 year weighing at least 15 kg.12,13 In pediatric patients with EoE, dupilumab may be considered as a second-line or subsequent therapy for those with persistent disease despite dietary modification and/or swallowed topical corticosteroids. In select cases, such as children with significant comorbid atopic diseases, including asthma, atopic dermatitis, poor tolerance of dietary restrictions, or contraindications to steroids, it may be used earlier in the treatment course through shared decision-making (Figure 2).3
Esophageal dilation is reserved for rare pediatric cases with fibrostenotic disease causing dysphagia or food impaction.9 Strictures caused by long-standing inflammation are uncommon in pediatric EoE. However, in rare cases, dilation using Savary or balloon dilators may be considered.14 Esophageal dilation is used in pediatric patients after other treatments have failed.15
Long-term management and interdisciplinary care
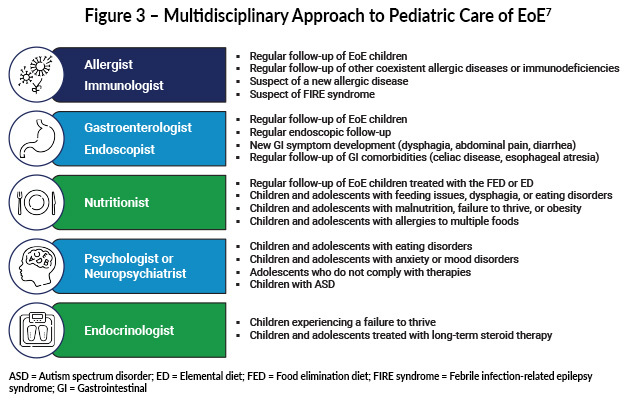
There is no single preferred therapy for EoE, and treatment decisions should be individualized based on age, disease severity, lifestyle, comorbidities, and family preferences, using shared decision-making.3,4 Optimal pediatric care is multidisciplinary, involving pediatric gastroenterologists, allergists/immunologists, registered dietitians or nutritionists, speech/feeding therapists when indicated, and primary care providers to address growth, feeding behaviors, and allergic comorbidities.16-19 This approach supports nutritional adequacy, growth, psychosocial well-being, and long-term disease control. (Figure 3)

Resources
Pediatric-focused clinical guidance and family education resources for eosinophilic esophagitis.
American Academy of Pediatrics (AAP). https://www.aap.org/en/patient-care/eosinophilic-esophagitis/
Professional education and clinical resources for the diagnosis and management of EoE.
North American Society for Pediatric Gastroenterology, Hepatology & Nutrition (NASPGHAN). https://naspghan.org/professional-resources/medical-professional-resources/eosinophilic-esophagitis/
Evidence-based guidelines and clinical toolkits for EoE management across age groups.
American Gastroenterological Association (AGA). https://gastro.org/clinical-guidance/guideline-toolkits/eosinophilic-esophagitis-toolkit/
Patient and caregiver education on EoE and its overlap with allergic conditions.
Asthma and Allergy Foundation of America. https://aafa.org/programs/education-programs/asthma-allergies-patient-caregiver-webinars/eosinophilic-esophagitis-eoe-webinars/
Patient-friendly resources to improve awareness and understanding of eosinophilic esophagitis.
SeeEoE. https://www.seeeoe.com/resources#resources-for-patients
Find a pediatric gastroenterologist.
NASPGHAN. https://members.naspghan.org/NASPGHANMembers/NASPGHANMembers/Find-a-PEDGI.aspx
References
- Chen JW. Management of eosinophilic esophagitis: Dietary and nondietary approaches. Nutr Clin Pract. 2020;35:835-847. doi:10.1002/ncp.10571
- Votto M, De Filippo M, Lenti MV, et al. Diet therapy in eosinophilic esophagitis. Focus on a personalized approach. Front Pediatr. 2022;9:820192. doi:10.3389/fped.2021.820192
- Dellon ES, Muir AB, Katzka DA, et al. ACG clinical guideline: Diagnosis and management of eosinophilic esophagitis. Am J Gastroenterol. 2025;120:31-59. doi:10.14309/ajg.0000000000003194
- Hirano I, Furuta GT. Approaches and challenges to management of pediatric and adult patients with eosinophilic esophagitis. 2020;158:840-851. doi:10.1053/j.gastro.2019.09.052
- Hirano I. Clinical relevance of esophageal subepithelial activity in eosinophilic esophagitis. J Gastroenterol. 2020;55:249-260. doi:10.1007/s00535-019-01624-3
- Durban R, Dellon ES. Nutritional care of the patient with eosinophilic esophagitis. Practical Gastroenterol. 2018;17:40-51. https://practicalgastro.com/wp-content/uploads/2019/07/Nutritional-Care-of-the-Patient-with-Eosinophilic-Esophagitis.pdf
- Votto M, De Filippo M, Caimmi S, et al. A practical update on pediatric eosinophilic esophagitis. Children. 2023;10:1620. doi:10.3390/children10101620
- Heine RG, Peters R, Cameron DJ, et al. Effect of a 4-Food elimination diet and omeprazole in children with eosinophilic esophagitis – A randomized, controlled trial. J Allergy Clin Immunol. 2019;143(2 suppl):AB309. doi:1016/j.jaci.2018.12.941
- Muir A, Falk GW. Eosinophilic esophagitis: A review. JAMA. 2021;326:1310-1318. doi:10.1001/jama.2021.14920
- Fable JM, Fernandez M, Goodline S, et al. Retrospective comparison of fluticasone propionate and oral viscous budesonide in children with eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2018;66:26-32. doi:10.1097/MPG.0000000000001626
- Dellon ES, Katzka DA, Mukkada VA, et al. Long-term safety and efficacy of budesonide oral suspension for eosinophilic esophagitis: a 4-year, phase 3, open-label study. Clin Gastroenterol Hepatol. 2025;23:2155-2166.e5. doi:10.1016/j.cgh.2024.12.024
- FDA Approves First Treatment for Eosinophilic Esophagitis, a Chronic Immune Disorder. PR Newswire. May 20, 2022. https://www.prnewswire.com/news-releases/fda-approves-first-treatment-for-eosinophilic-esophagitis-a-chronic-immune-disorder-301552266.html
- FDA Approves Dupixent As EoE Treatment For Children From One to Eleven, EOS Network, January 26, 2024. https://www.eosnetwork.org/news/fda-approves-dupixent-for-children
- FDA Approves Dupixent As EoE Treatment For Children From One to Eleven, EOS Network, January 26, 2024. https://www.eosnetwork.org/news/fda-approves-dupixent-for-children
- Al-Hussaini A. Savary dilation is safe and effective treatment for esophageal narrowing related to pediatric eosinophilic esophagitis. J Pediatr Gastroenterol Nutr. 2016;63:474-480. doi:10.1097/MPG.0000000000001247
- Katzka DA. Esophageal dilation as the primary treatment for eosinophilic esophagitis. Gastroenterol Hepatol (N Y). 2019;15:320-322. PMCID: PMC6676355
- Dellon ES, Gonsalves N, Hirano I, et al; American College of Gastroenterology. ACG clinical guideline: Evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol. 2013;108:679-692. doi:10.1038/ajg.2013.71
- Lucendo AJ, Molina-Infante J, Arias Á, et al. Guidelines on eosinophilic esophagitis: evidence-based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterol J. 2017;5:335-358. doi:10.1177/2050640616689525
- Chawla K, Alabbas B, Sheth D, Papademetriou M. As easy as EoE: A novel and effective multidisciplinary approach to care of patients with eosinophilic esophagitis in the age of biologics. Dig Dis Sci. 2020;65:2196-2202. doi:10.1007/s10620-020-06366-4
- Sauer BG, West A, McGowan EC. Multidisciplinary eosinophilic esophagitis care: A model for comprehensive patient-centered care through shared decision making between gastroenterology, allergy, and nutrition of the patient with eosinophilic esophagitis. Clin Gastroenterol Hepatol. 2021;19:2226-2229. doi:10.1016/j.cgh.2021.07.025
All URLs accessed on January 15, 2026